

Background: Coronavirus disease 2019 (COVID-19) appears to be associated with increased arterial and venous thromboembolic disease. These presumed abnormalities in hemostasis have been associated with filter clotting during continuous renal replacement therapy (CRRT). The incidence, clinical features, and treatment strategies to address severe filter clotting in patients with COVID-19 is unknown.
Aim: We aimed to characterize the burden of CRRT filter clotting in patients with COVID-19 infection and to describe a CRRT anticoagulation protocol that used anti-factor Xa levels for systemic heparin dosing.
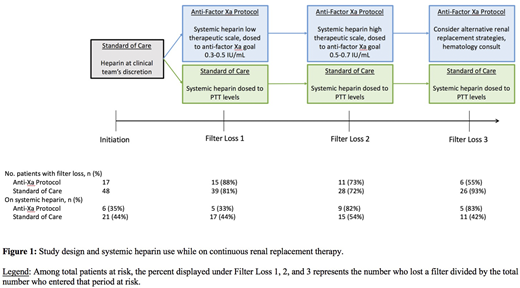
Methods: Consecutive patients with confirmed COVID-19 infection admitted between March 16, 2020 and April 27, 2020 who required CRRT were included in this multi-center retrospective study. Severe clotting was defined as >2 filter losses in 48 hours or one filter loss <8 hours into CRRT. Primary outcome was time to CRRT filter loss. Due to the unreliability of PTT levels in patients with COVID-19, a COVID-specific CRRT anticoagulation protocol (referred to as protocol henceforth) which dosed systemic unfractionated heparin (UFH) by anti-factor Xa levels was piloted at one center starting April 13, 2020.
Given that there was no difference in the treatment plan from CRRT initiation to first filter loss between the two anticoagulation approaches, this period served as a run-in period. Time from first to second filter loss (where protocol patients were exposed to low systemic UFH dosing) and time from second to third filter loss (where protocol patients were exposed to high systemic UFH dosing) were analyzed with a log-rank test.
Results: Sixty-five patients were analyzed, with 17 using the anti-factor Xa protocol to guide systemic heparin dosing whereas 48 were treated with standard of care anticoagulation dosed by PTT . There were no major differences between groups in age, sex, race, ethnicity, body mass index, or baseline medications. Fifty-seven out of 65 patients (88%) initiated CRRT for AKI, whereas 8/65 patients (12%) had end stage renal disease. At the time of CRRT initiation, 64/65 patients (98%) were mechanically ventilated, 22/65 patients (34%) required prone ventilation, and 59/65 patients (91%) were on intravenous vasopressors. Patients spent a median of 6 [2, 13] days on CRRT.
Fifty-four out of 65 patients (83%) lost at least one filter. Median first filter survival time was 6.5 [2.5, 33.5] hours. There was no difference between groups in percentage who lost their first filter (88% vs. 81%), or second filter (73% vs. 72%). However, fewer patients in the protocol group lost their third filter (55% vs. 93%) resulting in a longer median third filter survival time (24 [15.1, 54.2] vs. 17.3 [9.5, 35.1] hours, p = 0.04), Figure 1.
Conclusions: The rate of CRRT filter loss is high in COVID-19 infection. An anticoagulation protocol using systemic unfractionated heparin, dosed by anti-factor Xa levels is a reasonable approach to anticoagulation in this population.
Rosovsky:Bristol-Myers Squibb: Consultancy, Research Funding; Portola: Consultancy; Janssen: Consultancy, Research Funding; Dova: Consultancy. Sise:EMD-Serono: Research Funding; Abbvie: Research Funding; Gilead: Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Research Funding; Bioporto: Consultancy. Steele:HealthReveal: Consultancy; Blackstone Life Sciences: Consultancy. Czarnecki:Alexion: Consultancy; Reata: Consultancy. Allegretti:Mallinckrodt Pharmaceuticals: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal